A shared vision
This year’s dedicated Grand Challenge session was chaired by Liam Eaglestone, CEO of the Steve Morgan Foundation, alongside Professor Simon Heller, Chair of the Grand Challenge Scientific Advisory Panels.
First up was Professor James Cantley, who shared updates on his ambitious drug discovery work to help the body regenerate insulin‑producing beta cells destroyed by the type 1 diabetes immune attack.
Dr Cantley’s team have created a screening system that can quickly test thousands of drugs already used in people, looking for those that might help kick start beta cells into multiplying. They’ve already found several promising options, including drugs that switch off DYRK1A – a natural ‘brake’ on beta‑cell division. The most promising drugs are now being tested in mice to see if they can increase insulin production and help control blood sugar levels.
Building better scaffolds for beta cell replacement
Professor Vicky Salem was next, sharing her team’s approach to using biomaterials to protect beta cells from the immune attack in type 1 diabetes. Her group is developing a water‑based, jelly coating known as a hydrogel. This is designed to envelop transplanted lab‑grown beta cells, helping to hide them from immune attack. As well as acting as a protective shield, the hydrogel also helps the cells to connect to a blood supply, giving them the best possible chance to survive and thrive.
Professor Salem explained how the team has refined their approach. Earlier, thicker coatings helped shield beta cells but could affect how well they functioned. The team therefore went on to develop much thinner protective layers around the cells – termed nano-encapsulation. This ultra-thin coating still offers immune protection, while allowing oxygen and insulin to flow freely keeping the cells healthy. The team is now testing the benefit of including an additional layer of proteins into their coating as another way to protect the cells from the immune attack.
The long‑term goal is to develop a beta cell therapy that could be delivered via a simple injection, rather than surgery. The team is also using lab-based models to better understand how these protected cells behave once they are placed in the body.
Reflecting on the translational nature of the work, Professor Salem said:
“We’re behaving like a biotech – iterative, trial and error. There’s a lot of hope, but also a lot of fails.”
Why the small things matter in type 1 diabetes
Dr Teifion Luckett, a postdoctoral researcher presenting on behalf of Professor Sarah Richardson, shared insights into why type 1 diabetes often progresses more aggressively in young children.
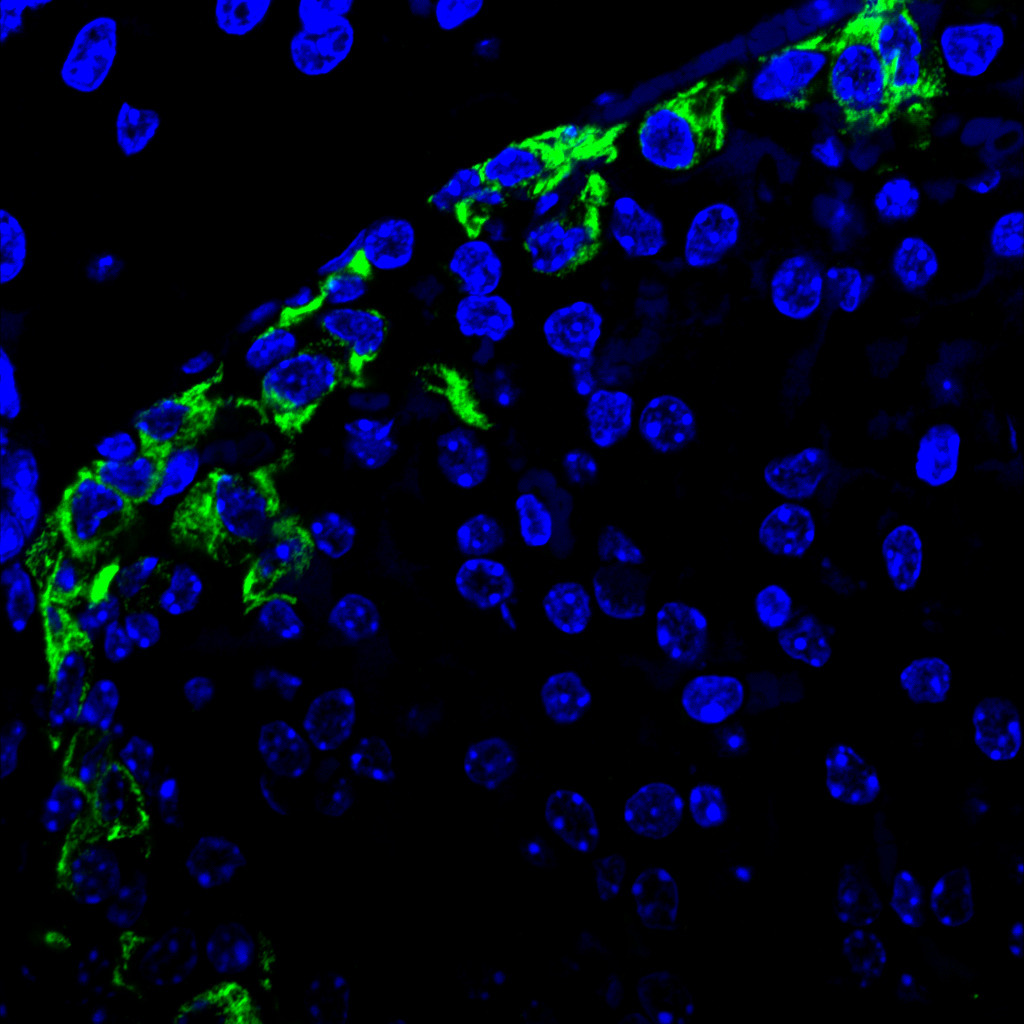
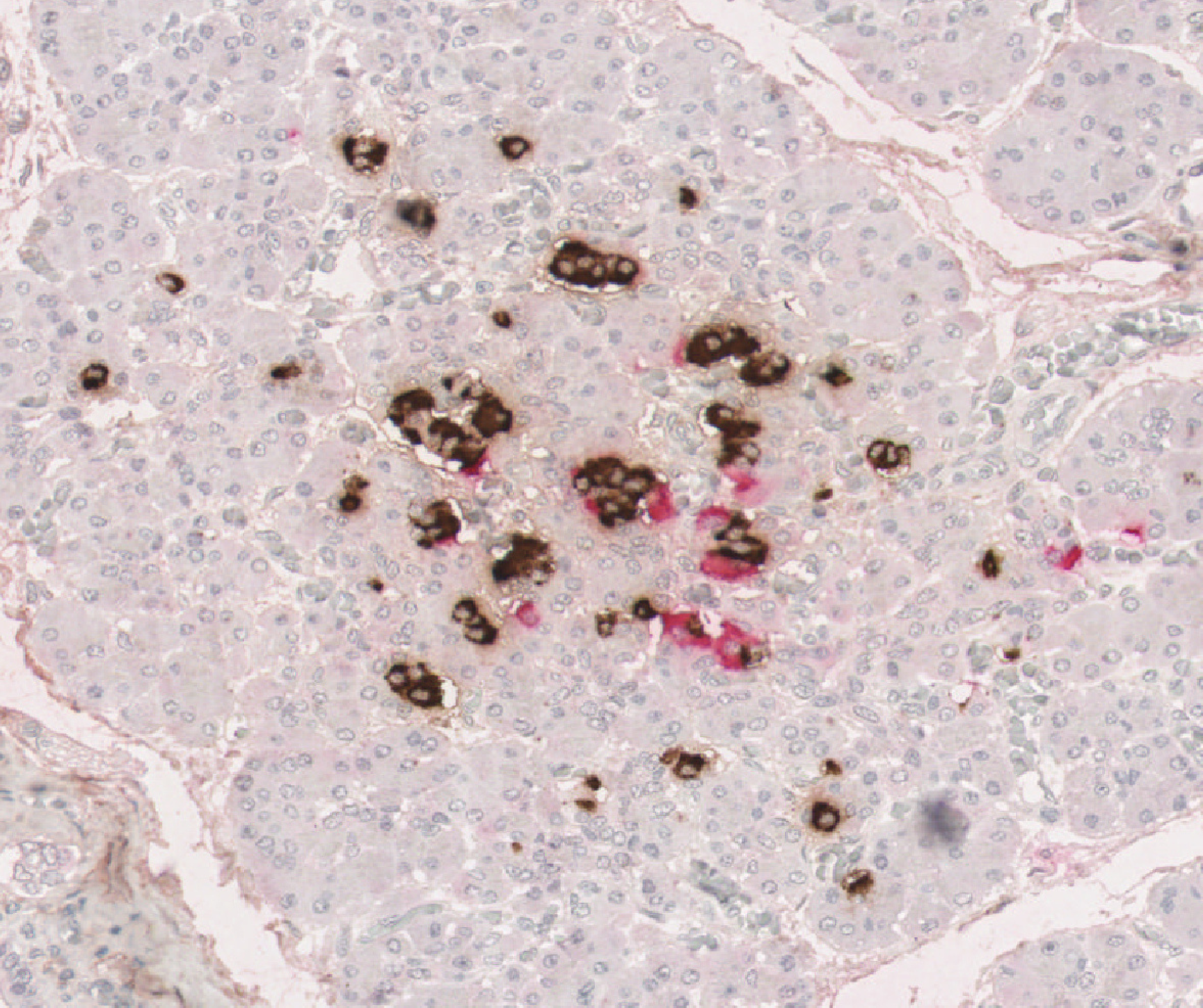
By studying rare human pancreas samples across different ages and stages of type 1 diabetes, the team identified clear differences between people with and without the condition. In early childhood, people without type 1 diabetes have many small clusters of beta cells, which normally grow and mature over time, with the most rapid development occurring in the first few years of life. In contrast, in people living with type 1 diabetes, these small clusters are almost completely absent – having been destroyed by the immune system early on. While some people living with type 1 diabetes retain a small number of larger clusters, this is not typically the case for those diagnosed in early childhood.
This early loss appears to be particularly important. The smallest clusters, once thought to be insignificant, are especially vulnerable to immune attack. Their rapid destruction prevents them from developing into larger, more resilient clusters, leaving very few insulin‑producing beta cells later in life. This helps explain why children diagnosed with type 1 diabetes at a young age often cannot produce any of their own insulin, making the condition harder to manage.
A smarter approach to insulin
The final update from the Grand Challenge session came from Professor Michael Weiss. He shared early but promising progress on a new type of ‘smart’ insulin that could help reduce the risk of dangerous low blood sugar in people with type 1 diabetes.
Low blood sugar is one of the biggest challenges of insulin treatment, as it can be dangerous and stressful to manage.
The research, published in 2025, focuses on a new type of insulin designed to respond more intelligently to the body’s needs. This new approach combines insulin with glucagon (a hormone that raises blood sugar) in a single, linked molecule. When blood sugar is too high, the insulin works as normal to bring it down. But when levels start to drop, the glucagon part of the molecule signals the body to release stored sugar, helping to prevent blood sugar from going too low.
His research has shown promising results in animal models, where both parts of the molecule worked as intended.
Early‑career researchers driving the future
The Early Career Awards session featured work from Grand Challenge researchers funded through the Beta Cell Therapy Programme Grant led by Professor Shanta Persaud and Professor Aileen King.
Dr Lydia Daniels Gatward received the Diabetes UK Early Career Investigator Award for her work on improving how well transplanted islets survive and function. Her research looks at how supportive biological ‘scaffolds’, together with mesenchymal stromal cells (MSCs – sometimes described as the body’s cellular handymen), can help islets release insulin more effectively and better cope with the stresses of transplantation.
Rosie Sullivan presented her PhD research investigating how helpful substances released by MSCs can improve the performance of lab‑grown beta cells once transplanted. Together, these projects showcase early career researchers as integral members of the Grand Challenge community, already making meaningful contributions while building careers as the future leaders of diabetes research.
Young Leaders in conversation
We were delighted to be joined by Young Leaders from Diabetes UK’s Together Type 1 programme, also funded by the Steve Morgan Foundation.
At DUKPC, Grand Challenge researchers and Young Leaders came together to explore how lived experience can help shape research. In one discussion, Young Leader Kamala asked Professor Craig Beall, a Grand Challenge‑funded researcher, what lived experience means to him and how it influences his work. Their exchange highlighted how insights from people living with type 1 diabetes help guide research priorities and impact across the Grand Challenge.
Reflecting on the conversation, Kamala said:
“It was really meaningful to hear directly from the people behind the research and to see just how much work, care and collaboration goes into the science.”
Looking ahead
At DUKPC we were delighted to learn that the Type 1 Diabetes Grand Challenge has been named a finalist for the Steve Morgan Foundation’s Long‑Term Impact Award. This recognition reflects the strength of the programme, bringing together cutting‑edge science, translational ambition and meaningful involvement of the type 1 community. The conference was a powerful reminder of why this work matters: its potential to transform how people with type 1 diabetes manage their condition, and the hope it brings for a cure.